ASSENT-4 PCI: Assessment of the Safety and Efficacy of a New Treatment Strategy for Acute Myocardial Infarction
Prior studies and a systematic review of large, randomized trials have shown that percutaneous coronary intervention (PCI) in the acute phase of myocardial infarction (MI) is superior to thrombolytic therapy. However, time delays for primary PCI are not insignificant and, as a consequence, only a minority of patients are actually treated within the 90-minute window recommended by current guidelines. Furthermore, previous studies have shown that early administration of fibrinolytic therapy is helpful and may be as efficacious as primary PCI.
The Assessment of the Safety and Efficacy of a New Treatment Strategy for Acute Myocardial Infarction (ASSENT)-4 PCI study was intended to be a large, randomized trial in acute MI patients facing very long delays (3-4 hours) before receiving therapy, as is typical for patients facing long travel distances or who must be transferred to a hospital with interventional facilities. The results of this study, including subanalyses, are presented below.
Study Design
ASSENT-4 PCI was designed to determine whether immediate fibrinolysis prior to delayed PCI would mitigate the negative impact of that delay and improve clinical outcomes. It was an open-label, 1:1 study that randomized patients to either full-dose full-dose tenecteplase (TNK-tPA) plus PCI (facilitated PCI) or to primary PCI with unfractionated heparin. PCI was to be performed between 60 and 180 minutes after randomization. Glycoprotein IIb/IIIa inhibitors were used either as a bail-out situation in patients pretreated with fibrinolytic therapy or at the investigators' discretion in the PCI-alone arm. Clopidogrel was administered only to patients who underwent stent implantation in both groups.
Primary Endpoint
Death, cardiogenic shock, or congestive heart failure within 90 days.
Inclusion Criteria
- Symptom onset within 6 hours prior to randomization
- Intention to perform primary PCI
- ST-segment elevation summation with a total of ≥ 6 mm
ASSENT-4 PCI: 90-Day Clinical Outcomes
Presenter: Frans Van de Werf, MD, PhD (University Hospital Gasthuisberg, Leuven, Belgium) on behalf of the ASSENT-4 PCI Investigators
In the study, which took place in 24 countries between November 2003 and April 2005, a total of 1667 patients were randomized to either facilitated PCI (n = 829) or PCI alone (n = 838) . The study was prematurely stopped by the Data and Safety Monitoring Board (DSMB) due to a significant disadvantage in patients randomized to the facilitated-PCI arm.
Time of onset of pain to randomization was similar in the facilitated-PCI and PCI-alone groups (135 vs 140 minutes, respectively; P = .55). There was a 7-minute difference between randomization to first balloon in favor of patients treated with PCI alone, but the difference did not reach statistical significance (115 vs 107 minutes, P = .69). In addition, a significantly larger percentage of patients in the PCI-only arm were concomitantly treated during the procedure with glycoprotein IIb/IIIa inhibitors (50.4% vs 9.5%, respectively; P < .0001).
The primary endpoint (death, cardiogenic shock, or congestive heart failure within 90 days) was significantly lower in the PCI alone group compared with the facilitated-PCI arm (13.7% vs 18.8%, respectively; P = .0055). Other individual endpoints also favored the PCI alone arm (Table). The significantly higher rate of stroke at 90 days in the facilitated-PCI group was mainly due to a significant increase in the rate of intracranial hemorrhage (Table).
Table. Individual Endpoints at 90 Days
| Endpoint | TNK + PCI (n = 829) | PCI Alone (n = 838) | P Value) |
|---|---|---|---|
| Death (%) | 6.7 | 5.0 | .14 |
| CHF (%)td> | 12.1 | 9.4 | .08 |
| Cardiogenic shock (%) | 6.1 | 4.8 | .27 |
| Reinfarction (%) | 6.1 | 3.5 | .02 |
| Repeat TVR (%) | 6.6 | 3.6 | .006 |
| Rehospitalization (for cardiogenic shock) (%) | 0 | 0.1 | 1 |
| Rehospitalization for other cardiac reasons (%) | 10.5 | 11 | .75 |
| Total stroke (%) | 1.81 | 0 | .004 |
| Intracranial hemorrhage (%) | 0.97 | 0 | .03 |
| Ischemic stroke (%) | 0.6 | 0 | < .0001 |
CHF = congestive heart failure; PCI = percutaneous coronary intervention; TNK = full-dose tenecteplase; TVR = target vessel revascularization
In addition, in-hospital major bleeding complication rates were similar in both the facilitated-PCI and PCI-only groups (5.7% vs 4.3%, respectively; P = .22), but there was a significantly higher rate of minor bleeding complications in patients treated with facilitated PCI (25.2% vs 18.9%, P = .002).
Conclusions
- In this prematurely terminated trial, the incidence of the combined clinical endpoint of death, congestive heart failure, or shock at 90 days was significantly higher in the facilitated-PCI arm than in the PCI-alone arm.
- The stroke rate in the facilitated-PCI arm was consistent with previous TNK trials but surprisingly low in the PCI-alone arm.
- Repeat target vessel revascularization and re-infarction were also reported more often in the facilitated-PCI arm.
- Therefore, a strategy of routine, immediate PCI following full-dose lytic, as used in this study population and with this protocol, cannot be recommended.
ASSENT-4 PCI: Subgroups and Angiography Analyses
Presenter: Allan M. Ross, MD (George Washington University Medical Center, Washington, DC)
The results presented by Dr. Ross focused on different subgroup analyses of this study.
Time to Therapy. Patients randomized to TNK had a 10-minute delay from randomization to treatment, whereas patients randomized to PCI alone had a delay of 107 minutes from randomization to first balloon. Therefore, there is a 97-minute difference between the 2 groups.
Mortality Over Time. Mortality was stable across different time periods in patients randomized to facilitated PCI, whereas in patients randomized to PCI alone, it increased between the time when the DSMB stopped the trial, at 30-day analysis, and at 90-day analysis (Figure 1).

Figure 1. Evolution of mortality.
Enrollment Site. Enrollment was performed mainly at hospitals with PCI facilities (46%); 35% of patients were enrolled in a non-PCI hospital, and 19% of patients were randomized in the ambulance.
Time From Onset of Pain to Randomization by Enrollment Site. The shortest time from pain to randomization was in patients randomized in the ambulance (105 minutes), whereas the longest was in hospitals with PCI facilities (160 minutes). In hospitals without PCI facilities, the time from pain to randomization was 130-135 minutes. Similar trends were observed in the time period from randomization-to-balloon time (ambulance 98 minutes; hospital with PCI facilities 140 minutes; and hospital without PCI facilities 95 minutes). Randomization time to thrombolysis was similar in the 3 groups (10-12 minutes).
Mortality by Site of Enrollment. Patients randomized at a hospital with a PCI facility and treated with facilitated PCI had the highest mortality, whereas the rate was lowest in patients randomized in the ambulance to facilitated PCI (Figure 2).

Figure 2. Mortality by site of enrollment.
Mortality by age was similar regardless of the treatment assignment.
Mortality by gender. Mortality in female patients treated with TNK plus PCI was almost double that of their male counterparts (Figure 3).

Figure 3. Gender and mortality.
Figure 3.
Mortality by Site of Infarct. Patients with anterior wall infarction and treated with TNK plus PCI had higher mortality rates than those treated with PCI alone.
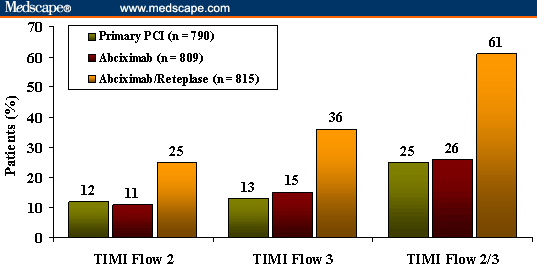
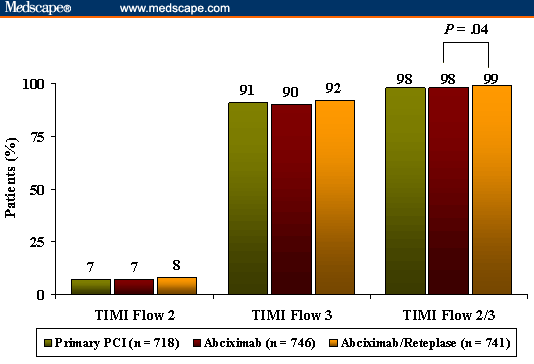
TIMI-3 Coronary Blood Flow. Normal TIMI-3 coronary blood flow at the diagnostic coronary angiography was observed in 43.5% of patients pretreated with TNK vs only 15.1% of patients treated with PCI alone. The rate of normal TIMI 3 coronary blood flow was highest in patients who underwent randomization and were treated in the ambulance (55%) and lowest in those treated at a PCI-facility hospital (33%). Following the procedure, a similar percentage of patients had achieved normal coronary blood flow (88%).
Conclusions
- Time intervals, place of enrollment, and lower than expected reperfusion rates in the facilitated-PCI group provide some insight into the results of this study.
- It remains unclear what impact fibrinolysis would have on outcomes in MI patients with truly long delays before intended PCI.
Commentary
ASSENT-4 PCI provides important data regarding facilitated PCI. The concept of initiating lytic therapy in patients who cannot undergo immediate PCI for a variety of reasons (lack of facility, lack of personnel, busy cath lab, etc) while they wait for intervention is appealing and seems to make sense. But like so many hypotheses in medicine, they do not always reflect reality. Patients treated with TNK prior to PCI had worse outcomes (increased stroke and mortality) than those patients who underwent PCI alone, to the extent that the DSMB had to stop recruitment.
The subgroup analyses presented by Dr. Ross are provocative and raise more questions regarding patients who may actually derive some benefit from this treatment (eg, those who receive treatment in the ambulance) vs those who may not (eg, female patients, those with anterior wall infarctions).
This study is in concordance with the Abciximab Before Direct Angioplasty and Stenting in Myocardial Infarction Regarding Acute and Long-term Follow-up (ADMIRAL)[1] trial, in which patients pretreated with abciximab in the ambulance actually derived the most benefit, whereas patients treated on-site did not.
The implications and the logistics of such treatment are complicated and would need to be assessed in a dedicated study.
Source:http://www.medscape.com/viewarticle/517566
Note: Some figures are not visible clearly. View them from original source.