The FINESSE and CARESS in AMI Trials: Is Facilitated PCI Ready for Prime Time?
Posted 12/20/2007
Luis Gruberg, MD, FACC
Author Information
Introduction
There are an estimated 500,000 new acute, ST-segment elevation myocardial infarctions (STEMI) events in the United States each year. A series of landmark studies has shown that prompt opening of the infarct-related artery is the treatment of choice in patients with STEMI, and this can be achieved either with drugs (lytics) or using a mechanical approach, such as percutaneous coronary intervention (PCI). Rapid reperfusion in combination with adequate pharmacologic treatment has been shown to reduce infarct size, minimize myocardial damage, and therefore decrease mortality rates in these patients. Primary PCI has been shown to be a superior strategy compared with lytics when performed in a timely fashion (less than 90 minutes) by an experienced team. However, 60% to 70% of STEMI patients present to hospitals that are not equipped with the facilities to perform primary PCI. Therefore, only a minority of patients will undergo PCI (diagnosis to balloon time) in less than 90 minutes.
According to the American College of Cardiology/American Heart Association (ACC/AHA) STEMI Guidelines,[1] lytics are still considered a viable option in patients who present less than 3 hours from symptom onset, especially in instances when an invasive strategy may be delayed beyond the recommended time or when there is no such option. Patients who present after 3 hours to a hospital without PCI facilities can either be transferred to another hospital or be treated with lytics. An obvious offshoot of this approach has been the administration of lytics followed immediately by transfer for planned PCI, known as facilitated PCI. The rationale to this approach is that a significant proportion of patients would undergo recanalization of the infarct-related artery prior to PCI.
A number of studies have evaluated this pharmacoinvasive approach; one of the most important and most recent was the Assessment of the Safety and Efficacy of a New Treatment Strategy for Acute Myocardial Infarction (ASSENT)-4 PCI.[2] This trial was designed to determine whether immediate fibrinolysis prior to delayed PCI would mitigate the negative impact of that delay and improve clinical outcomes. ASSENT-4 PCI was an open-label, 1:1 study that randomized patients to either full-dose tenecteplase (TNK-tPA) plus PCI (facilitated PCI) or to primary PCI with unfractionated heparin. PCI was to be performed between 60 and 180 minutes after randomization.[3] The study was terminated prematurely due to worse outcomes in patients randomized to the facilitated arm. The primary endpoint (death, cardiogenic shock, or congestive heart failure within 90 days) was significantly higher in the facilitated-PCI arm compared with the PCI alone group (18.8% vs 13.7%, respectively; P = .0055) (see Related Links). Other individual endpoints also favored the PCI-alone arm. However, other studies, such as Which Early ST-elevation Myocardial Infarction Therapy (WEST)[3] study and the Leipzig experience,[4] showed conflicting results. The mixed results between these studies warranted additional randomized trials.
At the recently held European Society of Cardiology 2007 World Congress in Vienna, Austria (see Related Links), 2 new important studies that assessed the role of facilitated PCI were presented: the FINESSE and CARESS in AMI trials. They are described below.
Final Results of the FINESSE Trial
Presenter: Stephen Ellis, MD, The Cleveland Clinic (Cleveland, Ohio), for the FINESSE Investigators
FINESSE Study Design
The Facilitated Intervention With Enhanced Reperfusion Speed to Stop Events (FINESSE) trial enrolled patients with a new STEMI within 6 hours of pain onset with estimated time to cath lab of 1-4 hours. Patients were randomized in a double-blind, double-dummy fashion to either 1 of 3 treatment strategies:
|
Patients were treated with aspirin and heparin and then transferred to the cath lab; patients in primary PCI received in-lab abciximab, and the facilitated PCI groups received placebo in the cath lab.
Primary endpoint: Composite at 90 days of all-cause mortality/rehospitalization for congestive heart failure, resuscitated ventricular fibrillation more than 48 hours after randomization, and cardiogenic shock.
Secondary endpoints:
|
Safety endpoints:
|
Results
Study enrollment was stopped due to budgetary issues in December 2006 after 2452 patients were entered into the study. A total of 1693 patients were enrolled in the main study and 759 in the low-molecular-weight heparin substudy. Baseline characteristics are shown in Table 1 .
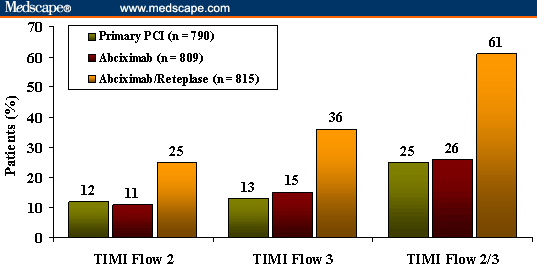
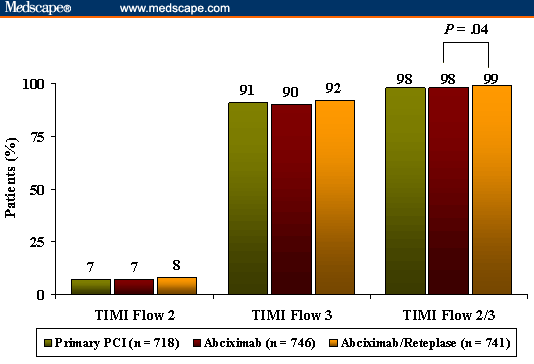
The average door-to-balloon time was 132 minutes. TIMI flow 2/3 prior to PCI was achieved in 61% of patients treated with reteplase/abciximab vs 25% in the primary PCI group and 26% in the placebo/abciximab group (Figure 1). TIMI flow 2/3 at the end of the procedure was achieved in 98% to 99% of patients in all 3 groups, and the rate was significantly higher in the reteplase/abciximab group compared with the abciximab facilitated PCI group (P = .04) (Figure 2). ST-segment resolution (> 70%) prior to balloon inflation was significantly better in patients treated with reteplase/abciximab. However, at 60-90 minutes after balloon inflation, ST-segment resolution was similar in all groups (Figure 3).
|
| Figure 1. (click image to zoom) FINESSE: TIMI flow in infarct-related artery before PCI. |
|
| Figure 2. (click image to zoom) FINESSE: TIMI flow in infarct-related artery after PCI. |
|
| Figure 3. (click image to zoom) FINESSE: ST-segment resolution before and after PCI. |
At 90 days, there was no difference in the primary composite endpoint between the 3 groups ( Table 2 ). There was also no difference in the rate of major secondary endpoints between the groups. However, total amount of TIMI bleeding complications was significantly higher in the facilitated PCI arms. There was also a higher rate of intracranial hemorrhage in the reteplase/abciximab group compared with the other 2 groups, but the difference was not significant.
FINESSE Conclusions
|
Clinical Outcomes in the CARESS in AMI Trial
Presenter: Carlo Di Mario, MD, PhD, Royal Brompton Hospital and Imperial College (London, United Kingdom), on behalf of the CARESS in AMI Investigators
The Combined Abciximab Reteplase Stent Study in Acute Myocardial Infarction (CARESS in AMI) study compared a strategy of early transfer of patients to a PCI center after thrombolysis vs medical treatment continued in the admitting hospital and transfer for rescue PCI only if there was evidence of lack of reperfusion. Patients less than 12 hours from symptom onset and with STEMI were randomized to either:
|
All patients were treated with aspirin, clopidogrel (started in the cath lab), heparin, reteplase, and abciximab.
Primary outcome: Death/reinfarction/refractory ischemia at 30 days.
CARESS in AMI Results
A total of 600 patients were randomized to facilitated PCI (n = 297) or to the medical/rescue (n = 300) arms of the study. The time from pain onset to reteplase treatment was 169-171 minutes. The time from reteplase administration to PCI was 136 minutes in the facilitated arm vs 212 minutes in the rescue arm. Baseline characteristics of patients enrolled in the study are shown in Table 3 .
Prior to PCI, TIMI 3 flow was observed in 60% of patients, and after the procedure, TIMI 3 flow was seen in 91% of patients. The length of hospital stay was greater in the medical/rescue arm. Only 55% of patients in the rescue arm were treated with a thienopyridine vs 85% in the facilitated arm. The combined endpoint of death/reinfarction/refractory ischemia at 30 days was significantly lower in the facilitated arm compared with the medical/rescue-treated patients (4.1% vs 11.1%, respectively; P = .001) ( Table 4 ). The individual endpoints are shown in Table 4 . Safety outcomes showed a significantly higher rate of bleeding complications in the facilitated arm of the study .
CARESS in AMI Conclusions
|
Viewpoint
On the basis of results obtained from these 2 important studies, at the present time we cannot make a clear-cut recommendation regarding the routine use of facilitated PCI in patients with STEMI. ASSENT-4 and FINESSE -- 2 very well-designed, important, and large studies -- failed to show a benefit, and results from ASSENT-4 suggest that the strategy may even yield a harmful effect. However, we cannot ignore the fact that in both studies a significantly higher percentage of patients achieved reperfusion (TIMI 2/3) in the infarct-related artery by the time they arrived to the cath lab. This is a critical observation when we consider that time is muscle. However, these findings still leave us questioning why the improved reperfusion rates did not translate to improved clinical outcomes. Possible explanations include an increase in bleeding complications, the lack of adequate antithrombotic/antiplatelet adjuvant therapy in ASSENT-4, or that perhaps these studies were underpowered to show a clinical benefit in a short period of time (30-90 days). Will the beneficial effect be evident at long-term follow-up?
The current guidelines of the ACA/AHA/SCAI for PCI have classified facilitated PCI as a Class IIb indication and stipulate that the technique could be performed as a reperfusion strategy in higher-risk patients when PCI is not immediately available and bleeding risk is low (Level of Evidence: B).[5] Although we may be somewhat reluctant, at the present time there is no clear indication for the routine use of facilitated PCI in STEMI patients, with the exception of high-risk patients in whom a long delay may be expected prior or during transport to a PCI facility.
Source: http://www.medscape.com/viewarticle/563069_1
No comments:
Post a Comment